The condition is quite common and affects 20% of the general population. The onset often occurs in childhood and can last for many years tending to decrease with age.
The cause is not fully understood, but it involves a T cell-mediated immune response induced by various triggers. A variety of factors are capable of triggering the development of mouth sores such as food ingredients or oral hygiene products, blood deficiencies, local trauma, stress, hormonal influences or genetic predisposition. In many cases, however, no specific cause can be identified.
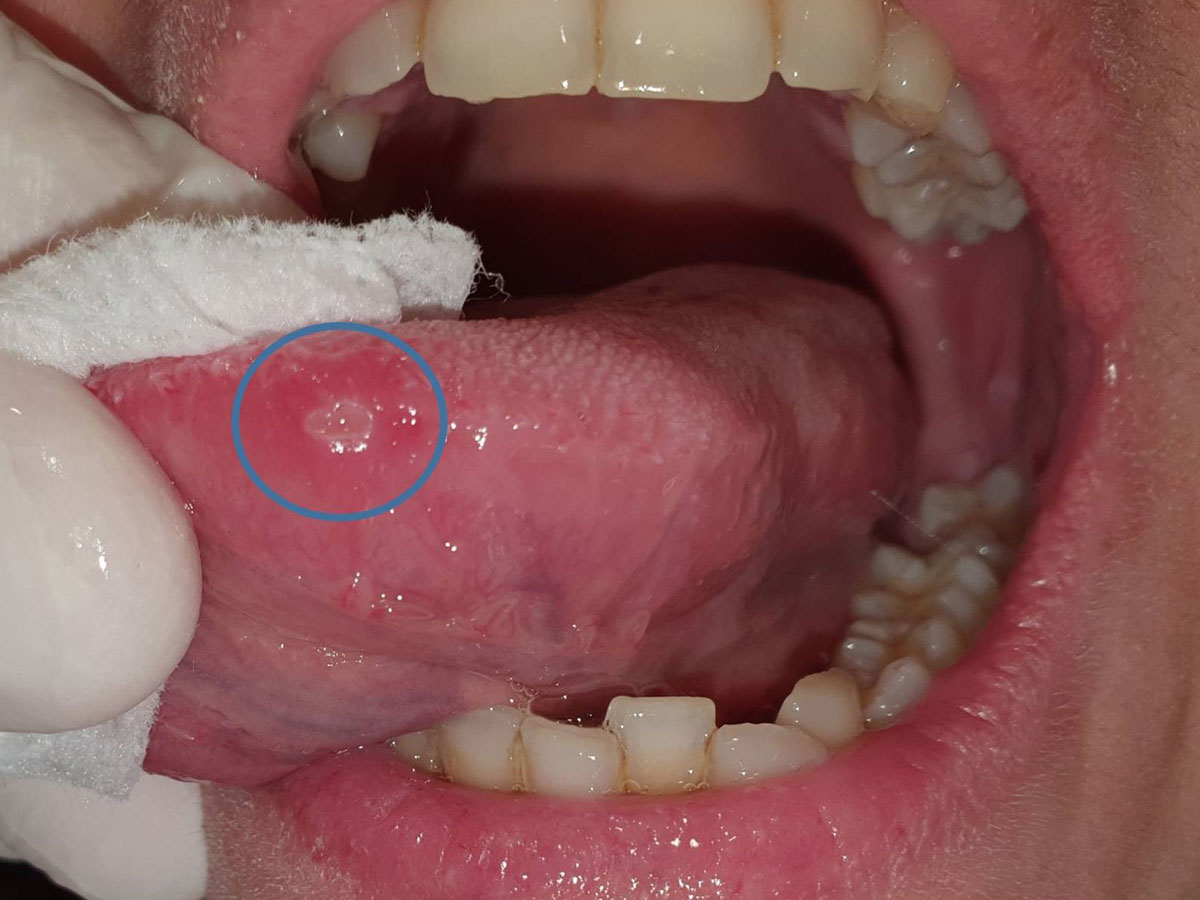
An aphthous ulcer is oval or circular in shape, covered by a pale yellow pseudomembrane, surrounded by a red halo and classified according to clinical criteria into three types: 1. common aphthous ulcers less than 10 mm in diameter that heal within 1-2 weeks and are the most common form ( 80%), 2. large aphthae with a diameter of more than 10 mm and taking weeks or months to heal often leaving a scar, and 3. herpetic ulcers, which are multiple, a few mm in size and disappear within a few weeks.
Lesions occur unpredictably, with asymptomatic periods, whilst the number of relapses per year may vary even in the same individual. Ulcers usually occur on the non-keratinized surfaces of the oral mucosa and the symptoms range from mild discomfort to severe pain during drinking or eating, leading to weight loss due to malnutrition in severe cases.
There is no definitive treatment, however, it is possible to suppress or even reduce the appearance of aphthae and the accompanying symptoms.