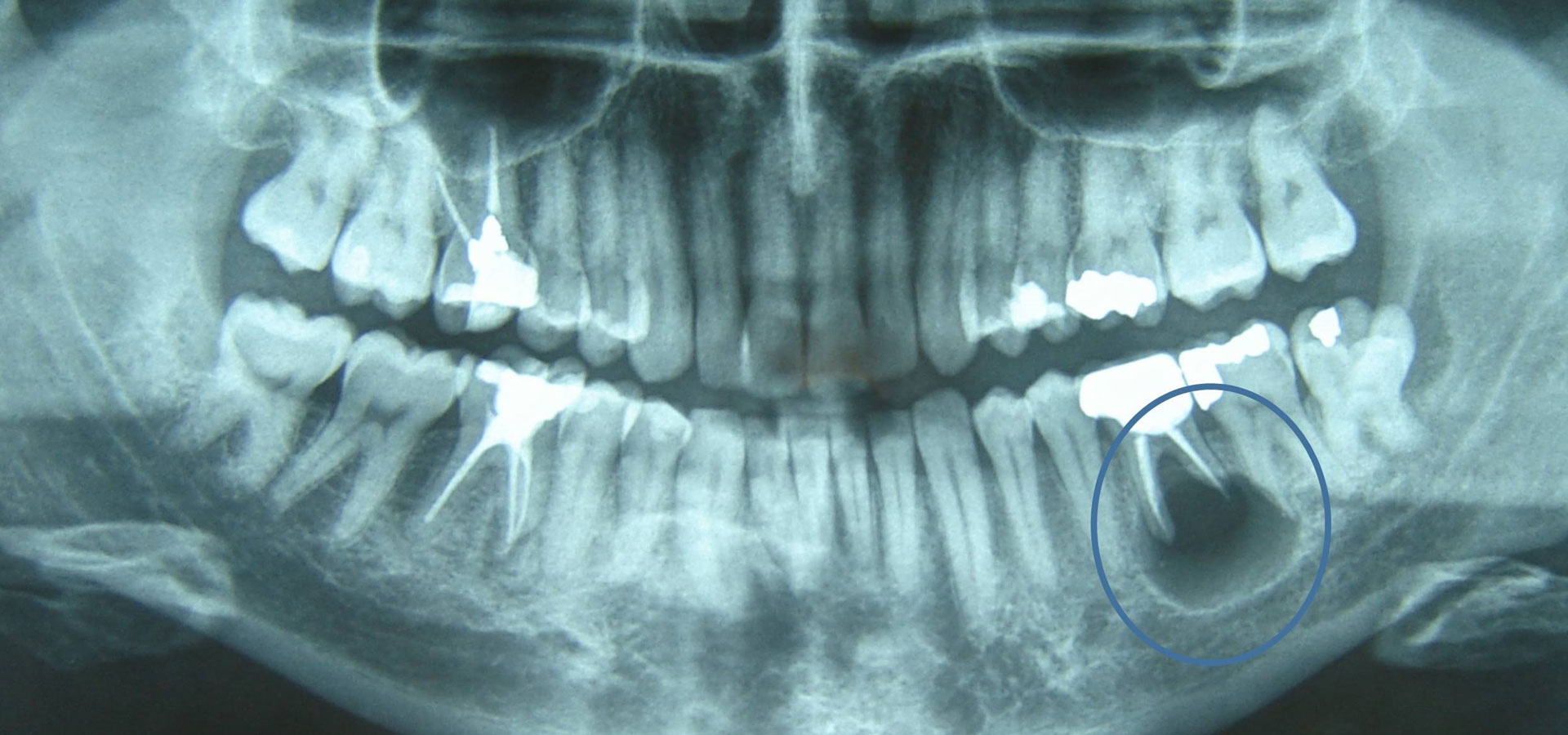
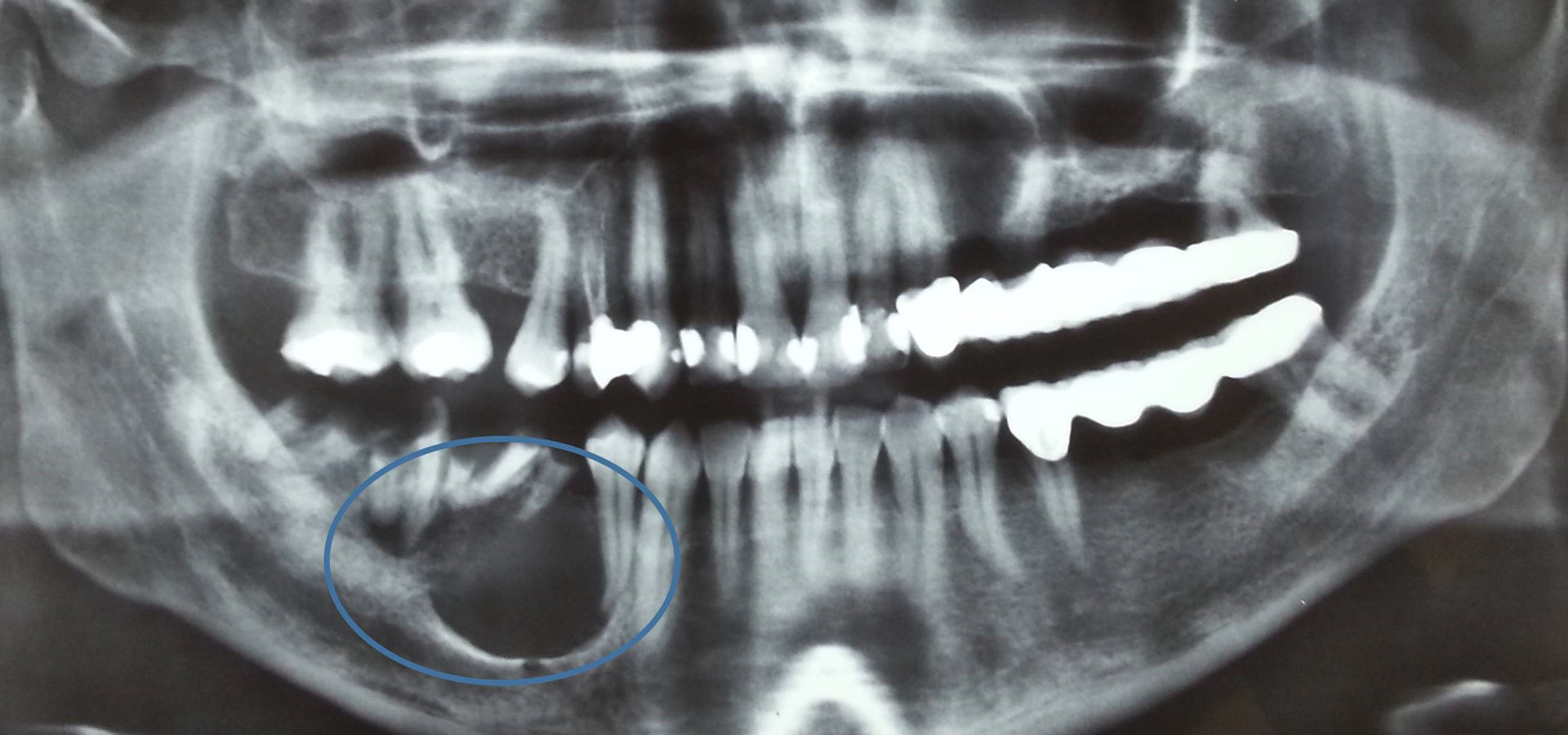
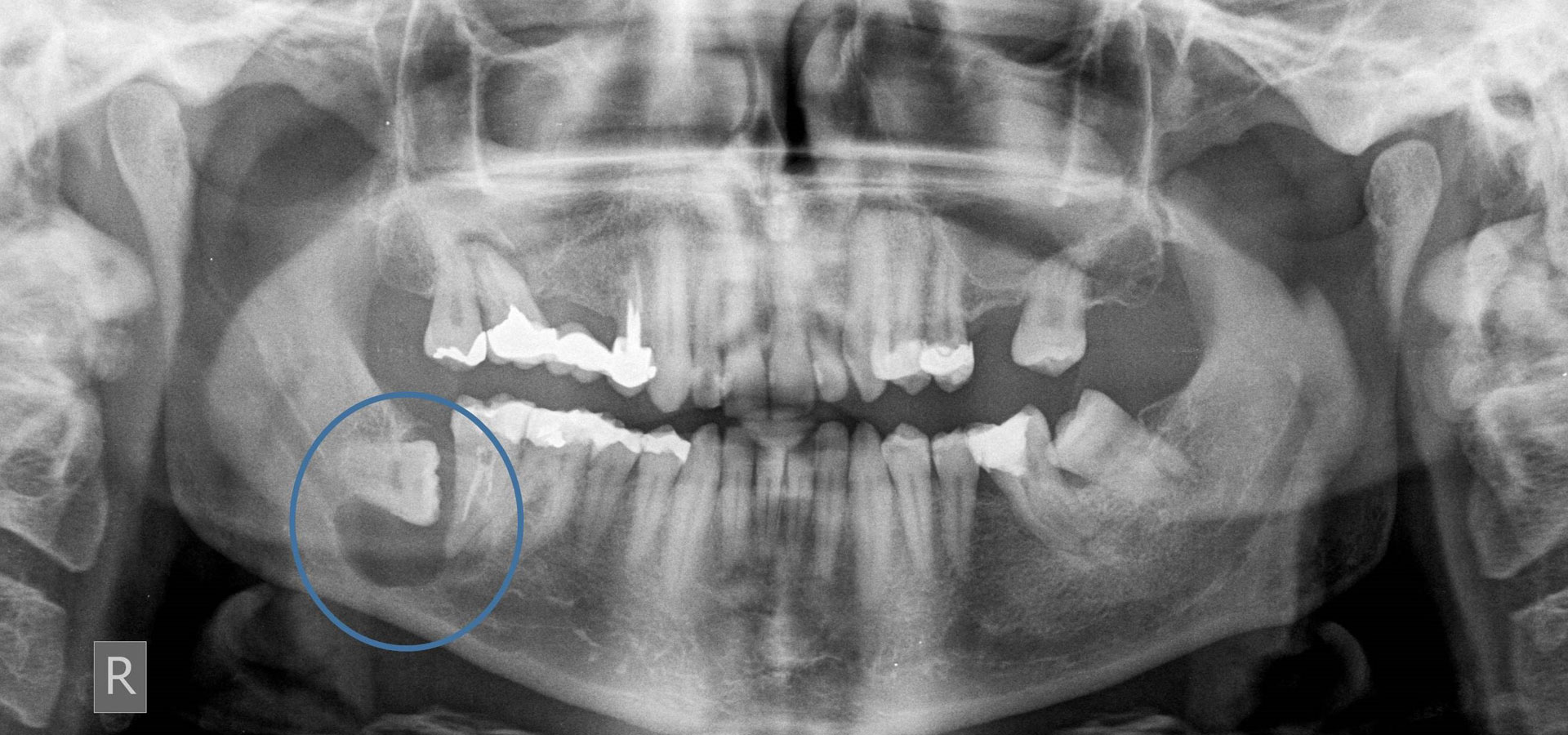
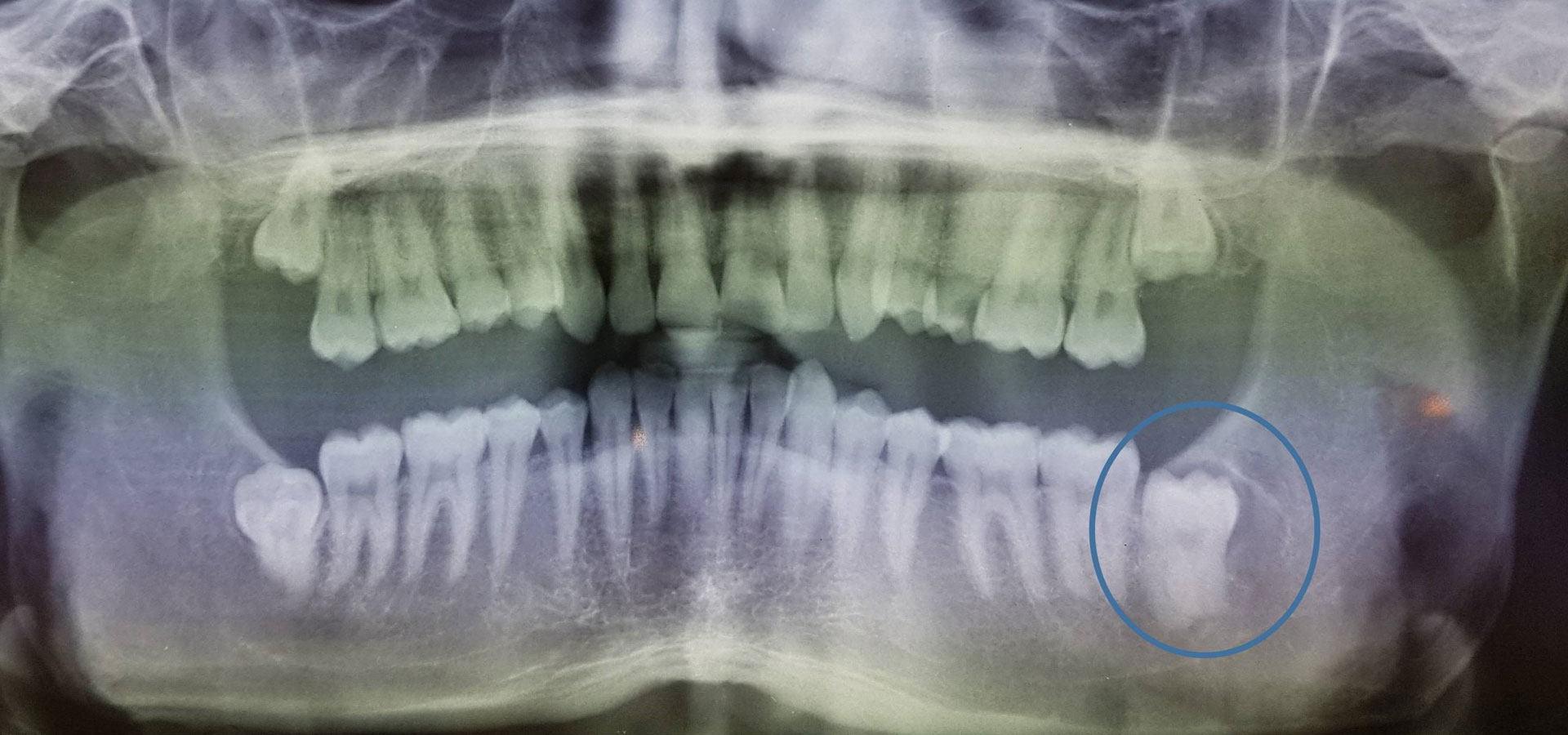
The most common cause of the development of a cystic cavity is inflammation, essentially due to microbes that are an aggravating factor for the growth and development of such a lesion. The most common inflammatory cyst is the radicular cyst that usually develops on the root periphery of inflamed teeth. Another relatively common cyst of developmental etiology manifests around impacted or semi-impacted teeth and is called a dentigerous cyst. Of course there is a wide range of cystic entities that will not be further analyzed here as this goes beyond the requirements of this text.
The reasons that cysts need to be treated are that these abnormal cavities, which can sometimes remain asymptomatic for a long time, gradually grow and expand into both adjacent teeth and anatomical entities, effectively destroying a larger area of tissues and structures. The result is that the teeth in the area lose bone support over time, while in cases of a great bone destruction it is possible pathological fracture of the jaws or neurological symptoms (e.g. numbness) in certain areas of the face may appear, due to damage of nerve branches. Of course, the possibility of abscesses and accompanying developing symptoms is always present, rendering the condition a medical emergency.
In regards to diagnosis a detailed clinical examination is required and in the case of any soft tissue involvement, an additional ultrasound examination is necessary, while in an intraosseous cyst, an appropriate radiological examination is needed. Additional data requiring evaluation are the study of previous radiographs and the vitality of the adjacent teeth.
The treatment of cystic lesions aims at the complete elimination of the lesion in order to inhibit its further development so that the affected areas return, as far as possible, to the previous structural and functional state. The surgical techniques that are mainly applied include enucleation, meaning the complete removal of the lesion and marsupialization, where communication with the oral cavity is achieved with the aim of gradually reducing the size of the lesion. Each of the aforementioned techniques has specific indications therefore it is up to the supervising doctor to decide based on the data of the respective case. The wound is sutured and appropriate postoperative instructions are given in order to achieve the best possible outcome.
The final diagnosis of the cystic type is made by histological examination and a proper histopathology report.
An important element is the regular monitoring and radiological re-examination of the patient to ensure the healing of the affected area and to exclude the possibility of recurrence of the lesion.